Brightway technologies (Lahore/Rawalpindi) ,Has Medical equipment repair centers in Pakistan BWT repairing advanced dermatological devices and Medical devices
Dermatoscopes (handheld devices for skin lesion analysis)
Microdermabrasion Machines
Radiofrequency (RF) Devices
UV Phototherapy Units
Hydrafacial Machines
High-Intensity Focused Ultrasound (HIFU)
Biopsy Punches
Electrocautery Devices
Fractional Laser Systems
LED Light Therapy Devices
Skin Resurfacing Machines
Pulsed Dye Lasers
Derma Rollers/Microneedling Devices
Spectrophotometers (for skin tone analysis)
Skin Analyzers (digital imaging systems)
CoolSculpting Machines
Chemical Peel Applicators
Portable Dermatology Kits
Why Choose Us ....?
Expert Technicians They follow strict protocols to ensure safety and quality assurance in every repair.
Genuine Parts We use 100% original or high-grade compatible replacement parts, sourced directly from trusted suppliers to maintain equipment performance and longevity.
Quick Turnaround Time We know how crucial equipment is to your clinic’s success. Our team ensures most repairs are completed within 3–7 business days, depending on the complexity of the issue.
Affordable Pricing Our services are priced competitively without compromising on quality. We provide a transparent cost breakdown after equipment inspection—no hidden charges.
Nationwide Support Whether you’re in Lahore, Karachi, Islamabad, Peshawar, Multan, or any other city across Pakistan, you can ship your machine to us safely and receive it repaired with care.
Warranty Provided Enjoy 30 to 90 days of repair warranty on all components replaced. If any issue persists, we’ll make it right at no extra cost.
If You Want To Buy Medical Devices and Surgical Instruement Kindly Visit Our Store
Digital stethoscope is a modernized model of the conventional stethoscope that permits healthcare experts to electronically report, examine, and shop heart sounds and different body sounds. It gives several blessings over traditional stethoscopes, making it a treasured tool in the modern-day healthcare industry.
Digital Stethoscope Usage
Using a digital stethoscope within reason is trustworthy. Here's a short step-by using-step manual:
1. Place the earpieces to your ears and modify the quantity to a stage this is comfortable for you.
2. Connect the stethoscope to the tool by way of plugging it into the headphone jack or Bluetooth.
3. Turn on the tool and choose the mode you want to use, along with normal, amplified, or heart murmur.
4. Place the chestpiece at the affected person's chest, making sure that it is placed over the desired place.
5. Gently press down, permitting the coronary heart sounds to be transmitted through the chestpiece.
6. Listen to the heart sounds and another frame sounds via the earpieces.
7. If recording is essential, choose the document button and start taking pictures the sounds.
8. To forestall recording, press the stop button or turn off the device.
9. Analyze the recording, if necessary, the usage of the built-in software program or external software program.
10. Store the recording for your affected person's statistics for future reference.
Different digital stethoscope fashions come with varying features to beautify their overall performance and value.
Here are some of the maximum not unusual capabilities:
1. Noise cancellation: This feature filters out history noise, making it less complicated to hear the heart sounds without a doubt.
2. Amplification: Some virtual stethoscopes have amplification competencies, allowing users to increase faint sounds.
3. Storage talents: Many virtual stethoscopes have integrated memory or the capability to connect to outside devices for storing recordings. This lets healthcare experts review heart sounds at a later time or percentage them with other healthcare specialists.
4. Connectivity: Some virtual stethoscopes are Bluetooth-enabled, allowing clients to wirelessly be a part of them to their smartphones or drugs for recording and playback. 5. Connectivity: Some virtual stethoscopes are nicely right with telemedicine structures, allowing healthcare experts to remotely listen to coronary heart sounds in real-time.
6. Software integration: Some digital stethoscopes have software integration competencies, allowing customers to research and export recordings to digital health document structures.
There are numerous key blessings that digital stethoscopes offer over conventional stethoscopes:
1. Increased accuracy and overall performance: Digital stethoscopes allow for more accurate detection of heart sounds and other body sounds, mainly to step forward affected person results.
2. Digital storage: The capability to shop recordings digitally eliminates the want for bodily paperwork, making it less complicated to get admission to and proportion affected person statistics.
3. Telehealth capabilities: Telehealth platforms enable healthcare professionals to remotely pay attention to coronary heart sounds, saving time and facilitating remote consultations.
4.Data evaluation: Digital stethoscopes provide advanced software program integration talents that allow customers to research recordings, generate opinions, and song developments.
Overall, digital stethoscopes provide numerous benefits over conventional stethoscopes, improving the quality of healthcare furnished.
With their superior abilities, stepped forward accuracy, and connectivity alternatives, digital stethoscopes are rapidly becoming the preferred desire for healthcare professionals.
If You Want To Buy Medical Devices and Surgical Instruement Kindly Visit Our Store
The stethoscope is a medical device used in different aspects of the medical field by doctors, physicians, cardiologists, EMTs, veterinarians, medical practitioners, and other healthcare professionals for multiple purposes to diagnose patients. If you are curious to know about What are the uses of stethoscopes? Where can we use it? Then you are at the right place. We are going to discuss the – uses of stethoscopes.
A stethoscope monitors and diagnoses the condition or seriousness of a patient's disease early. Its versatility allows us to use it for multiple purposes with portable features.
So let's discuss some important uses of stethoscope.
1. Uses Of Stethoscope in Medical Education and Research
We found that it is used not only by healthcare professionals but also commonly used in education and research purposes by practitioners. Use to teach students how to differentiate between normal and abnormal sounds in their research while gathering data on sounds for various cases.
2. Stethoscope For Listening to Lungs Sound
The stethoscope is commonly used to assess the lung condition of a patient by listening to and differentiating normal and abnormal sounds.
So, the stethoscope's chest piece is placed on the chest or back to listen to the respiratory sounds. This sound produces insights about the Lung's health.
You must listen carefully to check for abnormalities like weez,ronki,crepts, stride, and reduced breath sounds during respiration.
Then, you differentiate between normal and abnormal sounds to diagnose respiratory issues like pneumonia, bronchitis, asthma, etc.
The stethoscope is an effective asset for the timely diagnosis of any respiratory issue and treatment for healthcare professionals.
3. Listening to Heart sound
Cardiologists often use stethoscopes for listening to heart sounds produced during the opening and closing of heart valves. We can find disorders in valve functionality by using a stethoscope.
We must distinguish between normal and abnormal sounds like lub-dub, Heart murmurs during auscultation, and irregular or irregular rhythm sounds.
So, a stethoscope tells us about our heart health diseases like leakage or heart valve closures.
4. Used in detecting Bruits
We use it to detect bruits, a strange sound produced due to blood flow through blood vessels.
These sounds can indicate issues in blood vessels like atherosclerosis or stenosis, the narrowing of blood vessels. As blood flows through the vessels, Bruit sounds due to these issues that a stethoscope can detect.
5. To monitor fetal heart rate
We use it to monitor Fatal heart rate during pregnancy to assess the baby's health and well-being. A special type of stethoscope known as a Fetoscope monitors fetal heart Rate. The normal range of fatal heart rate is between 110 to 160 BPM(Beats Per Minute).
6. Use for emergency medication
Emergency doctors commonly use the stethoscope to make quick decisions and treatments by listening to lung, heart, and other internal body sounds. It helps doctors diagnose abnormalities earlier than a patient may exhibit those symptoms.
7. Can be used as a Hearing Aid
Stethoscopes are not specially designed to be used as hearing aids, but individuals with mild hearing impairment may find them helpful. It amplifies certain external sounds due to its design in certain situations.
However, it does not work in every situation as it is not designed to fulfill hearing loss needs, so it is better to consult an audiologist who can assess your needs and give appropriate solutions.
8. Used to hear Bowel sound
A stethoscope measures bowel sounds or abdominal sounds produced due to movement of air, fluid, or food and contraction or relaxation of the intestine. A stethoscope allows us to measure these sounds to diagnose abnormality by placing a chest piece on the patient's abdomen to hear bowel sounds.
Lack of bowel sounds may occur after surgery in certain conditions, and we might hear loud sounds in patients with diarrhea. So, a stethoscope effectively detects abdominal issues by hearing bowel sounds.
9. Used to monitor recovery rate after surgery
During recovery after surgical procedures and anesthesia, patients often experience slow-down bowel movements, discomfort, and reduced aptitude. Listening to that sound helps professionals monitor the patient's recovery status and any abnormality during recovery in a friendly way without discomfort.
So, doctors can adjust a patient's diet according to the situation.
10. Used a stethoscope in veterinary care
Veterinarians widely use a human stethoscope to diagnose abnormalities in animals, like cardiac and respiratory issues, detect abdominal problems, and listen to fatal heartbeats during pregnancy in large animals like cows, horses, etc. Veterinarians can use it for regular accusation to assess the overall health of animals.
11. In measuring blood pressure
The stethoscope monitors blood pressure, mostly in manual blood pressure machines. We use sphygmomanometer (cuff), and a stethoscope to measure blood pressure in a blood pressure monitoring machine.
The doctor uses a stethoscope to analyze the sound while releasing the cuff slowly lis, listening to the heartbeat, and analyzing systolic and diastolic pressure.
Tips on How to Use Stethoscope Effectively
To listen Accurately and for better auscultation, it’s important to use a stethoscope properly.
So, below are some tips for using a stethoscope.
Choose a good quality stethoscope, such as an acoustic or an electronic stethoscope, for precise diagnosis.
Set the patient in a comfortable position, such as listening to heard sounds lying down, and sitting up is better for lung sounds.
Clean your stethoscope with a disinfectant wipe or alcohol swap before use for infection control.
Put the earpiece in-ear with comfort and place the chest piece on the patient’s body.
Don’t press too hard on the patient. Place it gently and listen to the sound carefully. You hear
Diagnose issues by differentiating between normal and abnormal sounds.
Move the chest piece to different areas to listen to abnormal sounds.
Practising makes it easy to differentiate between normal and abnormal sounds, and you can also use a stethoscope effectively with time and experience.
Summary
Not only in humans, but we can also use it for animals to check recovery after surgery and overall health. We found that a stethoscope is widely used to measure blood pressure.
We must choose a quality stethoscope with good acoustic performance to diagnose the problems in the early stages.
A Stethoscope Impact is a diagnostic device medical professionals like doctors and nurses use to listen to sounds inside human and animal bodies. It consists of a y-shaped earpiece at one end and a chestpiece at the other with a diaphragm and bell.
A chest piece is placed on the patient's body to listen to sounds like heart, lung, abdominal, and other internal body sounds.
Closeup of a stethoscope isolated against a blue table
Before the invention of the stethoscope, doctors used to put their ears on the patient to listen to the internal sounds of the body.
In some conditions, doctors feel uncomfortable when they put the ear on overweight patients due to external Noise Interference.
Evolution of the Stethoscope Impact from paper to electronic
In 1816, a French physician named "Rene Laennec" came up with a solution and invented it for the first time.
He was in a situation where he had to check the chest sounds of a female patient and felt uncomfortable placing his ears directly. He folded a piece of paper and rolled it into a circle.
Then, He placed one end on the patient's chest and put his ear on the other end of that folded piece of paper.
After that, he replaced that paper with a wooden tube, and the design and structure were refined later as time passed.
As time passed, the designs of stethoscopes also changed, and now we have different types of stethoscopes with unique features.
What are the Types of Stethoscope Impact
These are some types
1. Acoustic Stethoscope Impact
These traditional stethoscopes used by medical professionals are portable, lightweight, and easy to carry. Use the traditional method by placing a chest piece on the patient's body to listen to internal sound.
They are suitable for general physical diagnosis of the patient's body due to listing a wide range of inner sounds,
We observe that Doctors, medical practitioners, nurses, EMTs(Emergency Medical Technicians), and surgeons commonly use these.
Further, we have two types that include
Dual-Head
2. Single -Head
2. Electronic Stethoscope Impact
Electronic stethoscopes are more costly than traditional ones due to their advanced features and electronic components, such as batteries.
They have built-in amplifiers that amplify the sounds louder to make them audible.
These have advanced features such as recordings and playback to hear the sound later.
Unlike traditional stethoscopes, electronic stethoscopes use electrical signals produced due to the conversion of vibrations with a microphone inside a chest piece.
We can modify these signals according to our requirements.
3. Fatal Stethoscope Impact
They are also known as Doppler stethoscopes, specially designed to listen to the heartbeat of a fetus during pregnancy.
It uses ultrasound technology to detect and amplify the heart sounds.
3. Cardiology stethoscopes
We often use them to listen to cardiac sounds, such as murmurs and irregular rhythms, with enhanced acoustic capabilities.
4. Padriatic stethoscope
We primarily use these stethoscopes while diagnosing children to listen to their internal body sounds. Specially designed with a small size chest piece and diaphragm to fit children's bodies best.
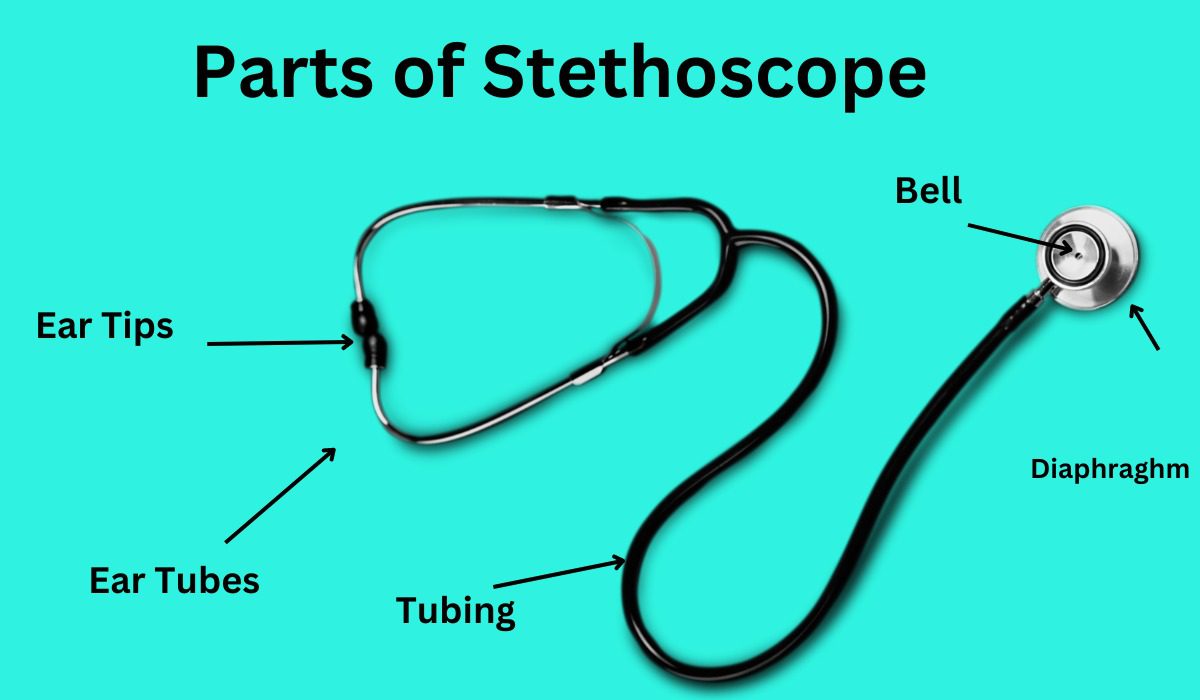
What are the Parts of Stethoscope:
Below are the different components of a stethoscope.
Earpiece
These are the part of the stethoscope that goes into the ears of a healthcare professional. Designed to provide comfort to the ear and minimize external noise while listening to the internal organs of the patient's body.
Tubing
Tubes that connect the earpiece with the chestpiece are flexible and hollow inside and transmit sound between the earpiece and the chestpiece. Tubing allows professionals To listen to body sounds comfortably and without fear of breakage.
Chestpiece
The chestpiece connected at the opposite end of the earpiece and placed on the patient's body to listen to internal sounds. It consists of two sides, including a diaphragm and a Bell.
Diaphragm
The diaphragm is a flat circular surface inside the stethoscope to listen to high-frequency sounds such as lungs, heart, and bowel sounds. It vibrates when placed on the patient's body due to the internal sound of the body and sound transmitted through the tubing toward the ears.
Bell:
Most of stethoscopes have both bell and diaphragm parts in the chest piece. Used to detect and listen to low-frequency sounds in the body that might not listen by using the diaphragm. It detects sounds like certain heart murmurs, blood flow sounds in arteries, and bowel sounds with a low pitch.
Tuneable Diaphragm
A tunable diaphragm is commonly used in modern stethoscopes 3M Litman stethoscopes instead of a bell and diaphragm. It has advanced features that allow us to easily listen to low and high-frequency sounds by adjusting the pressure to be applied to the chest piece.
Y-shaped tubing
To keep the sound separate from each ear, Y-shaped tubes are used. One end of the tube connects to each earpiece, and the other couples with a single tube of chest piece through tubing connectors.
The critical question is, can we buy these parts in Pakistan? The answer is yes, and we can easily buy these parts in Pakistan at the best price of Rs 6,280/-.
Summary
In conclusion, the stethoscope is an essential diagnostic device commonly used by medical professionals for different needs and was first invented by Rene Laennec in 1816 while he was listening to the heartbeat of a female. Then, the design and structure refined with time, and now we have electronic stethoscopes used to listen to babies' heart-beat even before they were born. There are different types of stethoscopes according to their need, and we can also buy their parts in Pakistan.